- Hold the fan about 6 inches (15cm) from your face or the distance you find most helpful
- Aim the cool air at your cheeks, nose and mouth.
- Either hold the fan still or move it around slightly, whatever you find most helpful.
From Bringing Breathlessness into View – a guide to living well with breathlessness: hyms.ac.uk
Watch “Using a handheld fan to reduce breathlessness” on YouTube
“Would you be surprised if the patient died within the next year ?”
– If NO then consider the following…
- Advance Care Planning
- Gold Standards Framework
- ReSPECT Forms
- Refer to palliative care team
“Breathing should be through the nose, using the diaphragm and done slowly. “Nose, low and slow”
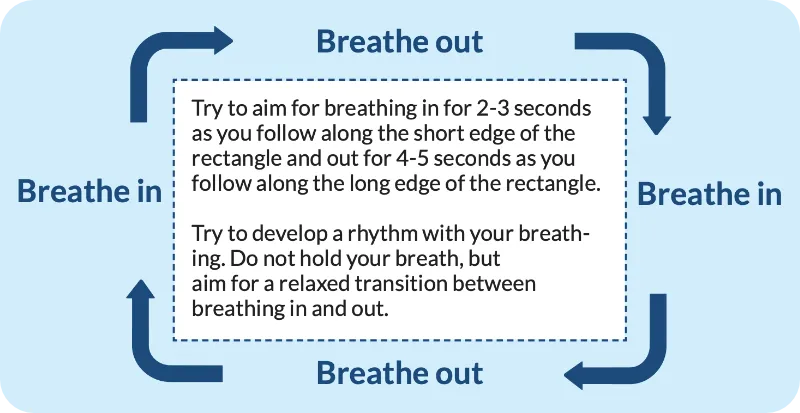
- Breath in
- Breath out
- Breath in
- Breath out
Try to aim for breathing in for 2-3 seconds as you follow along the short edge of the rectangle and out for 4-5 seconds as you follow along the long edge of the rectangle. Try to develop a rhythm with your breathing. Do not hold your breath, but aim for a relaxed transition between breathing in and out.
For more information: physiotherapyforbpd.org.uk
Grade 1
Are you ever troubled by breathlessness except on strenuous exertions?
Grade 2
Are you short of breath when hurrying on the level or walking up a slight hill?
Grade 3
Do you have to walk slower then most people on the level? Do you have to stop after a mile or so (or after 1/4 hour) on the level at your own pace?
Grade 4
Do you have to stop for breath walking about 100 yards (or after a few minutes) on the level?
Grade 5
Are you too breathless to leave the house, or breathless after undressing?